

Abstract
Background: Patients with severe hemophilia A experience substantial morbidity and mortality due to frequent spontaneous and traumatic bleeding episodes, especially in joints. Prophylaxis with standard half-life factor VIII (FVIII) is the standard of care to prevent bleeds. Extended half-life products benefit patients by reducing the number of infusions without impacting the treatment efficacy.
Methods: This phase 3b, prospective, open-label, multicenter, continuation study (NCT# 01945593) investigated the safety and efficacy of a PEGylated recombinant FVIII with an extended half-life, rurioctocog alfa pegol (SHP660, BAX 855, ADYNOVATE®, Shire, Lexington, MA, USA), for prophylaxis and treatment of bleeding in patients with severe hemophilia A (FVIII <1%). Eligible children and adults were ≤75 years of age and had either completed a previous rurioctocog alfa pegol study (NCT# 01599819, 01736475, 02210091, 02615691, 01913405, or 02585960) and were willing to immediately transition to the continuation study, or were naïve to rurioctocog alfa pegol but had received treatment with plasma-derived or recombinant FVIII for ≥150 (in patients ≥6 years of age) or ≥50 (in patients <6 years of age) exposure days. Patients received prophylactic rurioctocog alfa pegol at least twice weekly, either at a fixed dose (FD; 45 ± 5 IU/kg in patients ≥12 years of age; 50 ± 10 IU/kg in those <12 years of age; dose adjustment ≤80 ± 5 IU/kg allowed) or with pharmacokinetically (PK)-tailored dosing (≤80 ± 5 IU/kg) to maintain FVIII trough levels ≥3%. The co-primary endpoints assessed were the incidence of FVIII inhibitory antibody development (as measured by ≥0.6 BU in the Nijmegen modification of the Bethesda assay) and the spontaneous annualized bleed rate (ABR). Secondary endpoints included overall hemostatic efficacy ratings and occurrence of adverse events (AEs).
Results: The study began in October 2013 and completed in March 2018. Overall, 216 patients receiving prophylaxis were eligible and included in the safety/full analysis dataset (≥1 dose received). Of these, 215 were male, the mean (SD) age at enrollment was 22.8 (15.7) years, the mean (SD) number of documented previous rurioctocog alfa pegol exposure days was 57.0 (39.6), the total ABR over 3-6 months prior to enrollment in the continuation study (including patients naïve to rurioctocog alfa pegol or receiving on-demand or prophylactic treatment with rurioctocog alfa pegol) was mean (SD) 4.7 (12.6), median (range) 0.0 (0-69). Most patients (206; 95.4%) had participated in a previous rurioctocog alfa pegol study. Overall, 215 patients received ≥1 dose in the FD regimen and 25 received ≥1 dose in the PK regimen. These patients received a mean (SD) of 1.72 (0.29) and 2.11 (0.61) prophylactic infusions per week, respectively, with a mean (SD) dose per infusion of 51.15 (8.11) IU/kg and 52.14 (17.03) IU/kg, respectively.
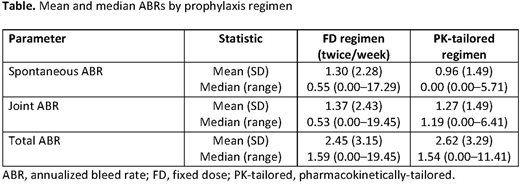
None of the patients developed a confirmed FVIII inhibitor in this study and only 1 treatment-related allergic or hypersensitivity reaction (a nonserious mild AE) was reported. Nonserious AEs assessed by the investigators to be related to treatment occurred in 11/216 (5.1%) patients. Serious AEs (SAEs) occurred in 33 (15.3%) patients; there were no SAEs assessed by the investigators to be related to treatment. Descriptive statistics on spontaneous, joint, and total ABR by prophylactic regimen are shown in the Table. The overall total ABR in all patients was mean (SD) 2.5 (3.1), median (range) 1.6 (0.0-19.5). Overall hemostatic efficacy was rated as good or excellent in 88.5% of all bleeds and 89.4% of all bleeds were treated with 1 or 2 infusions.
Conclusions: These results show that in previously treated patients with severe hemophilia A, rurioctocog alfa pegol prophylaxis in FD- and PK-tailored regimens was well tolerated and effective. None of the patients developed FVIII inhibitory antibodies, and a decrease in mean total ABR was reported in these patients compared with baseline.
Mullins:Shire: Honoraria, Membership on an entity's Board of Directors or advisory committees. Konkle:Genentech: Consultancy; CSL Behring: Consultancy; Gilead: Consultancy; Pfizer: Research Funding; Spark: Consultancy, Research Funding; BioMarin: Consultancy; Bioverativ: Research Funding; Shire: Research Funding; Sangamo: Research Funding. McGuinn:CSL Behring: Consultancy; BioMarin: Consultancy; Bioverativ: Membership on an entity's Board of Directors or advisory committees, Research Funding; Spark: Consultancy, Research Funding; Genentech: Consultancy; Shire: Research Funding; Pfizer: Research Funding. Engl:Shire: Employment, Equity Ownership. Tangada:Shire: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal